![[Blog] Investing in Africa’s Health: Unlocking Fiscal Space for Economic Transformation](https://www.uneca.org/sites/default/files/styles/slider_image/public/storyimages/shutterstock_2590924791_1920x640.jpg?itok=g61xjqgN)
By Nadia Ouedraogo, Aboubakri Diaw, Stephen Karingi *
From Input-Driven Growth to Productivity-Led Transformation: The Central Role of Health Financing in Africa
Over the past three decades, Africa’s economic expansion has been predominantly input-driven, propelled by labor force growth and the intensive use of natural resources rather than sustained efficiency gains and technological upgrading. While this model has delivered episodic growth—often during commodity booms—it has not generated the productivity improvements required for deep structural transformation. As a result, many African economies remain structurally vulnerable, with growth highly exposed to commodity price volatility, climate shocks, and tightening global financial conditions. Weak productivity dynamics have thus become a central constraint on Africa’s long-term development trajectory.
This constraint is becoming increasingly binding. Rapid population growth and accelerating urbanization are expanding the labor supply faster than productive employment opportunities, while fiscal space is narrowing under rising debt burdens and growing climate-related spending needs. In this context, growth strategies based on factor accumulation are reaching their limits. Sustaining growth, creating decent jobs, and raising living standards will require a decisive shift toward productivity-driven growth. For African economies, closing the productivity gap is therefore macro-critical.
At the core of this transition lies human capital. Productivity gains depend fundamentally on the ability of workers and firms to learn, adapt, and operate more efficiently. A workforce that is skilled, educated, and healthy supports improvements in production processes, enhances firm-level efficiency, and facilitates structural transformation. Without this foundation, increases in labor and capital yield diminishing returns.
Technology and innovation can accelerate these dynamics, but their impact depends on the quality of the underlying human capital base. Where skills, health, and institutional capacity are weak, technological adoption remains limited and generates limited spillovers. Conversely, stronger human capital enables effective absorption, adaptation, and diffusion of new technologies across sectors.
Health is therefore a foundational pillar of human capital. It shapes labor productivity, learning outcomes, and economic participation. Yet across Africa, health systems remain underfunded, fragmented, and heavily reliant on households and external financing. These constraints weaken human capital accumulation, limit productivity growth, and ultimately undermine the prospects for structural transformation.
From Health Financing to Structural Transformation
Building on this perspective, strengthening human capital requires sustained investment in health. Health is a central component of the productivity-enhancing process, directly shaping labor productivity, learning outcomes, and the capacity of individuals to participate in economic activity. Weak health outcomes reduce the returns to education and constrain the ability of economies to adopt and effectively use new technologies, while reinforcing inequalities in access to opportunities.
These outcomes, however, do not arise in isolation. They reflect the performance and accessibility of health systems, which determine the extent to which populations are able to sustain and improve their health over time. Where health systems are under-resourced, fragmented, or inaccessible, health outcomes deteriorate, limiting the accumulation of human capital and weakening the foundations for productivity growth.
Conversely, stronger and more inclusive health systems support better health outcomes, enhance workforce productivity, and improve resilience to economic and climate-related shocks. In this context, the way health systems are financed becomes critical, as it shapes their capacity, equity, and sustainability.
If productivity is the missing link between growth and structural transformation, and human capital its foundation, then health financing becomes a central pillar of economic strategy.
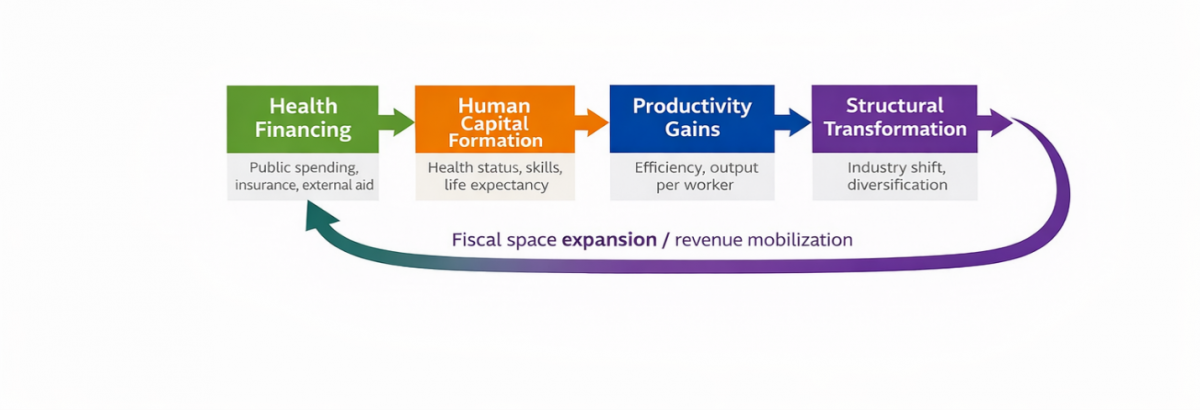
Figure 1 illustrates the transmission mechanism through which increased and more efficient health financing drives structural transformation. By strengthening health outcomes, it builds human capital, raises labor productivity, and supports the reallocation of resources toward more productive sectors.
Figure 1. From Health Financing to Structural Transformation: A Causal Pathway
A Structural Bottleneck to Productivity: Low and Unequal Health Investment
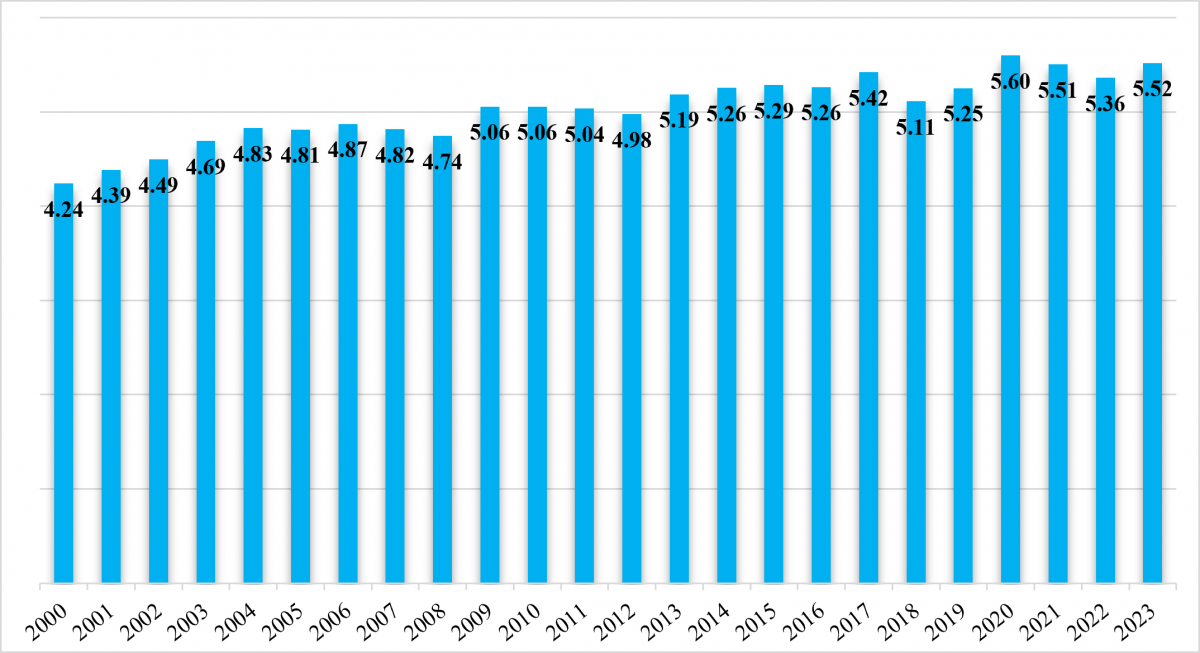
Health financing in Africa remains constrained both in scale and structure. Total health expenditure reached approximately US$143bn in 2023, representing only about 5.5% of GDP. This indicates that the health sector remains relatively small relative to the size of African economies and has not kept pace with rising demographic pressures and development needs.
Fig 2: Current health expenditure (CHE) as % Gross domestic product (GDP), 2023
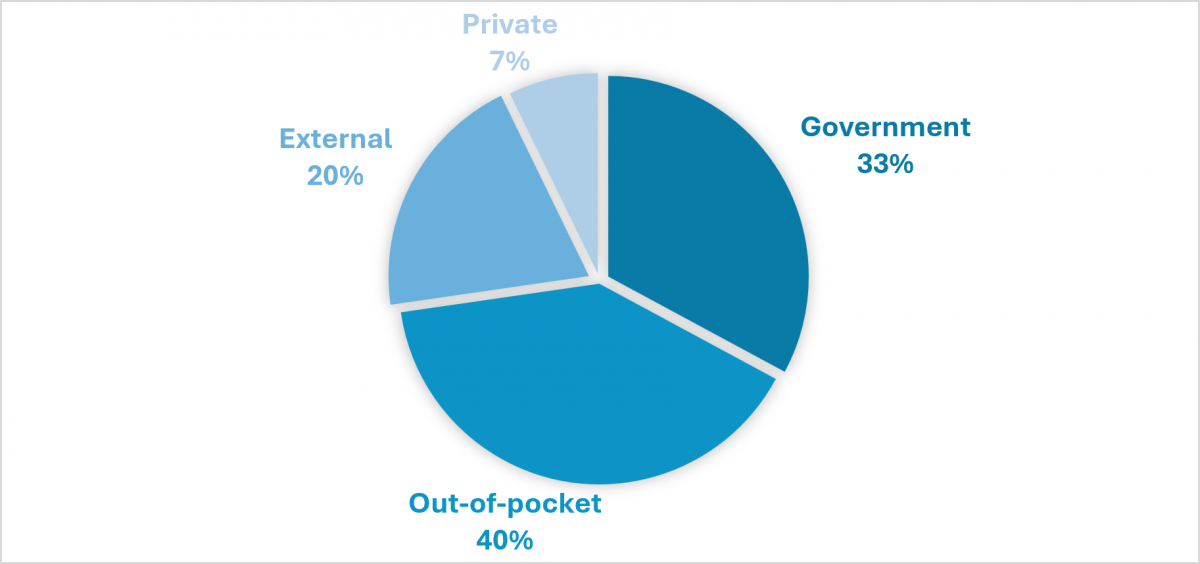
The challenge is not only the overall level of spending, but also its composition. Governments account for only 33%of total health expenditure, while the remainder is financed by households (40%), external partners (20%) and private contribution (7%). This limited public contribution reflects weak risk pooling and results in a heavy reliance on out-of-pocket payments, undermining financial protection.
Fig 3: Composition of Health Financing in Africa (Government vs Private vs External, 2023)
These constraints are reflected in low and highly unequal spending levels across countries. Per capita government health expenditure ranges from less than US$3 to over US$500, and the gap between the highest- and lowest-spending countries widened from US$416 in 2015 to more than US$535 in 2023.
Fig 4: Per Capita Health Spending Distribution Across African Countries in 2023
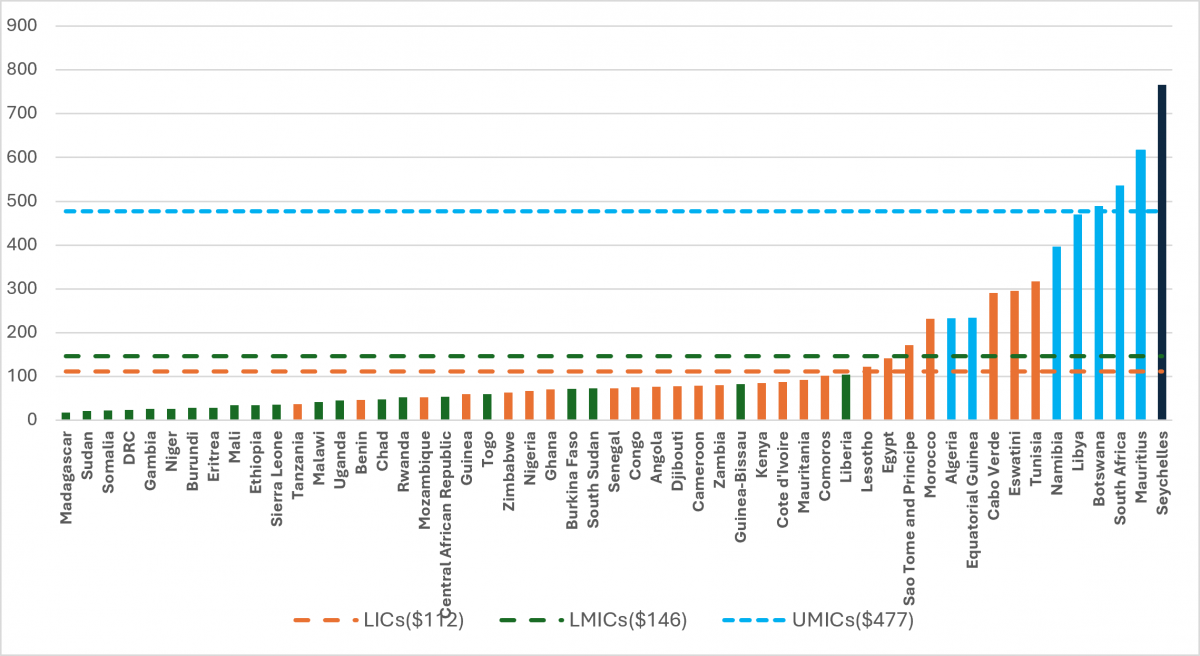
Importantly, a large share of countries remains below internationally referenced minimum spending levels required to deliver basic health services (often estimated in the range of US$100–150 per capita for essential service packages in low-income settings). This indicates that, beyond inequality, overall spending levels are insufficient to ensure adequate service coverage.
Overall, the limited scale of total health spending and the weak public financing base point to a structurally underfunded system, constraining the ability of countries to build resilient health systems and support productivity-enhancing human capital.
The Burden on Households: Financial Protection and Productivity Risks
In the absence of sufficient public financing, the burden of health spending shifts to households.
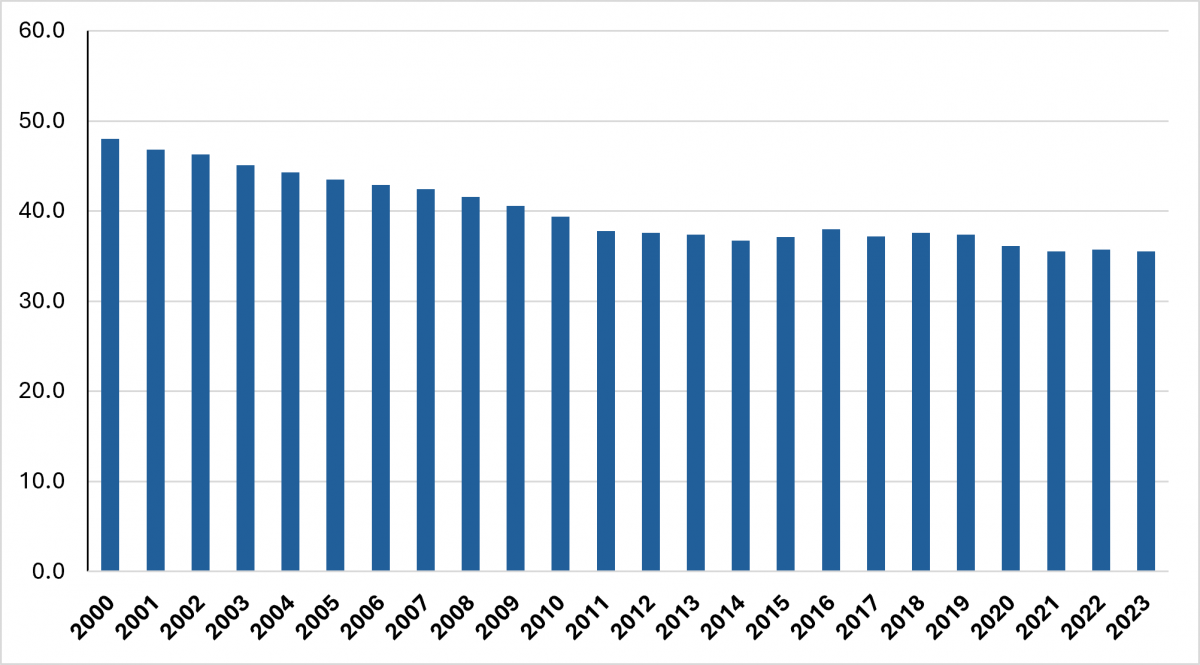
Across Africa, around three-quarters of countries exceed the 20% threshold for out-of-pocket (OOP) health expenditure—commonly used as a benchmark for financial protection—exposing households to a high risk of catastrophic health spending. On average, OOP payments account for about 36.7% of total health expenditure over the past decade.
Fig. 5: Out-of-Pocket Health Expenditure (% of CHE), 2023
The consequences are substantial. High out-of-pocket (OOP) costs lead households to delay or forgo care, deplete savings, and divert resources away from education and productive activities. These dynamics undermine labor productivity and perpetuate poverty cycles.
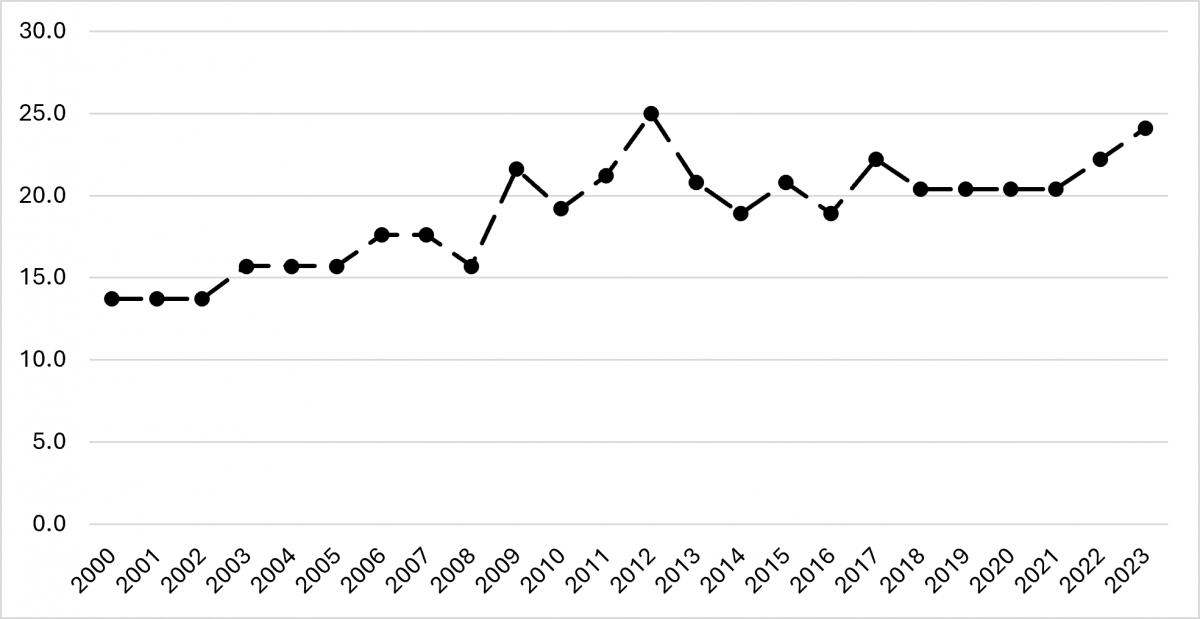
While some progress has been recorded, it remains limited. The share of countries meeting financial protection benchmarks increased from 13.7% in 2000 to just 24.1% in 2023. At the same time, more than one-third of households continue to face financial hardship due to health-related expenditures.
Fig. 6: Financial Protection Trends in Africa (2000–2023)
Fragmentation and Limited Risk Pooling: Limits to Systemic Transformation
Health financing systems in Africa remain structurally fragmented, limiting the effectiveness of spending.
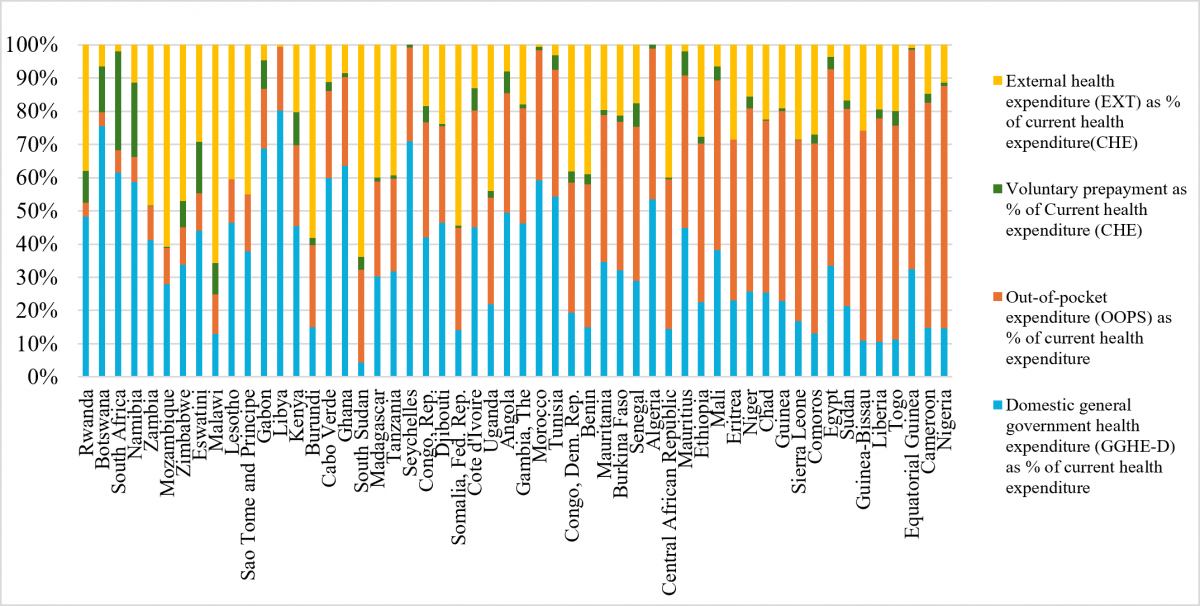
Public and prepaid mechanisms remain underdeveloped, while voluntary insurance contributes only about 4–5% of total health expenditure, indicating limited risk pooling. At the same time, dependence on external financing has increased—from 10.7% in 2000 to about 23.4% in 2023, raising concerns about sustainability and policy autonomy.
Fig. 7: Health Financing Structure by Source (% of CHE)
These patterns reinforce systemic inefficiencies, reduce the predictability of financing, and constrain the ability of health systems to allocate resources effectively.
These financing constraints have direct implications for progress toward Universal Health Coverage (UHC), which rests on two core pillars: service coverage and financial protection.
The evidence points to significant challenges on both fronts. High reliance on out-of-pocket payments and persistent financial hardship indicate weak financial protection. At the same time, low per capita spending and limited pooling mechanisms constrain the expansion of essential health services. As a result, progress toward UHC remains structurally constrained by the underlying financing architecture.
Fiscal Space as a Lever for Expanding Health Financing
The constraints observed in health financing systems ultimately reflect broader limitations in fiscal capacity. Expanding public investment in health therefore depends on governments’ ability to identify, mobilize, and allocate additional fiscal resources within existing macro-fiscal frameworks.
Assessing fiscal space is central to this process. It enables policymakers to identify potential sources of financing—through domestic revenue mobilization, expenditure reprioritization, and efficiency gains—and to determine how these can be sustainably directed toward health.
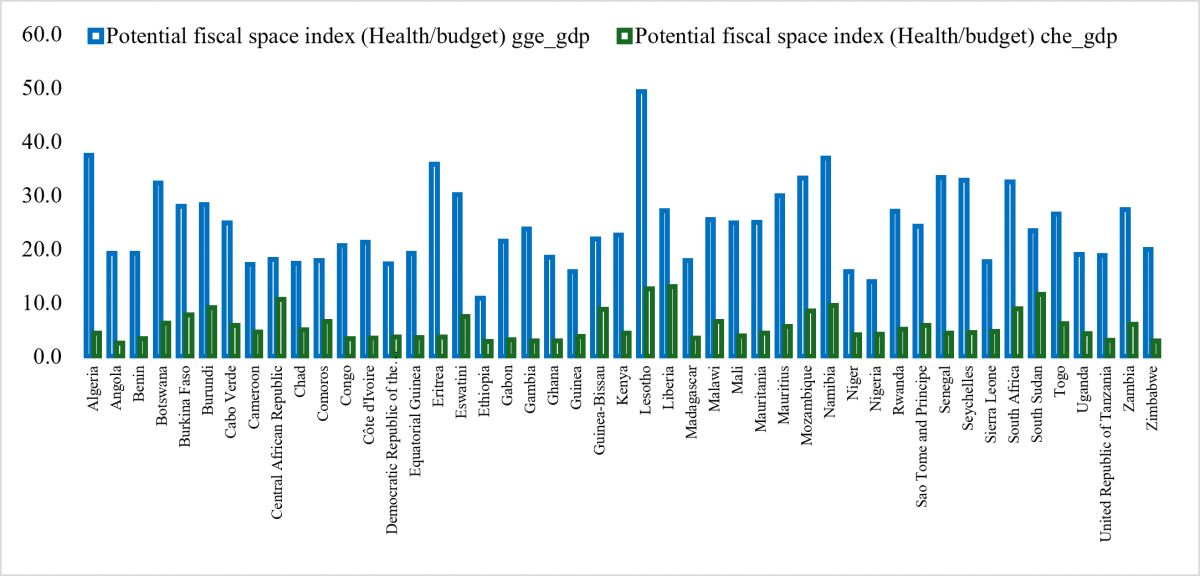
As illustrated in Figure 7, the scope for expanding fiscal space varies significantly across countries, reflecting differences in economic structure, revenue capacity, debt dynamics, and budgetary priorities. In some contexts, opportunities lie in strengthening tax systems and broadening the revenue base. In others, the priority is reallocating expenditure toward high-impact sectors such as health or improving the efficiency of existing spending.
Strengthening domestic resource mobilization remains particularly critical. Heavy reliance on external financing and out-of-pocket payments has proven both insufficient and unsustainable. A more robust fiscal foundation, anchored in predictable domestic revenues, is essential to support resilient health systems.
However, expanding fiscal space is not only about increasing resources. It also requires identifying the appropriate instruments and mechanisms through which this space can be created, stabilized, and sustained over time.
Fig 8: Potential Fiscal Space for Health Across African Countries.
From Fiscal Space to Financing Architecture
While expanding fiscal space is necessary, it is not sufficient. The critical next step is to translate this space into a coherent financing architecture that can mobilize diverse instruments and align them with country-specific realities, taking into account fiscal constraints, institutional capacity, and the level of financial market development.
In practice, this requires tailoring financing approaches to country contexts. Differences in economic structure, fiscal capacity, and institutional readiness imply distinct pathways for mobilizing and structuring resources. The following examples illustrate how countries can combine instruments—such as domestic revenue mobilization, expenditure reprioritization, and innovative financing mechanisms—to expand and sustain health investment in line with their specific constraints and opportunities.
Debt Instruments — Creating Predictable Fiscal Space
Debt instruments are a standard component of macroeconomic management, used to manage liabilities and smooth fiscal adjustment. Their relevance for health lies in their capacity to generate predictable fiscal space when appropriately structured.
In Ethiopia, currently undergoing restructuring under the G20 Common Framework, this creates a concrete opportunity. A portion of the debt service relief could be explicitly linked to multi-year health allocations within the national budget. Even modest reallocations can generate substantial and predictable financing flows over time, aligned with medium-term fiscal frameworks.
Levies — Anchoring Domestic Financing
Excise taxes and solidarity levies are well-established tools of domestic resource mobilization. Their strength lies not in scale, but in stability and predictability.
In Togo, for example, modest excise taxes on tobacco, alcohol, or sugar-sweetened beverages could generate revenues in the order of 0.2 to 0.5 percent of GDP annually. More importantly, such instruments establish a reliable domestic financing base, reduce dependence on out-of-pocket spending, and support more structured health financing systems.
Blended Finance — Addressing Risk Constraints
Blended finance responds to a central constraint in many African economies: not the absence of capital, but its cost and associated risk perceptions.
By combining concessional resources, guarantees, and public financing, blended finance enables more efficient risk allocation and can unlock investments that would otherwise not materialize. In Sierra Leone, where fiscal space is constrained and debt vulnerabilities are high, such instruments can catalyze initial investments in health infrastructure and service delivery, helping to establish a track record for scaling.
Institutional Investors — Mobilizing Domestic Capital
Institutional investors, including pension funds and insurance companies, represent a largely untapped source of long-term financing. However, their participation requires predictable returns, strong governance frameworks, and appropriate investment vehicles.
In Botswana, where financial markets are relatively developed, there is clear potential to channel a portion of domestic institutional capital toward health-related investments, including infrastructure, digital systems, and insurance mechanisms. Even small allocations can have significant catalytic effects.
Diaspora and ESG Instruments — Expanding the Financing Frontier
Beyond domestic sources, diaspora financing and ESG-linked instruments offer additional avenues for diversifying the financing base.
In countries such as Cabo Verde and Comoros, where remittances account for a substantial share of GDP, diaspora bonds could transform fragmented flows into structured investments—for example, financing hospital infrastructure or health insurance systems with clear returns and accountability mechanisms.
Similarly, ESG-linked instruments provide an opportunity to integrate health outcomes into capital market financing. Bonds linked to measurable improvements in service coverage or financial protection can reposition health as a performance-based investment, rather than purely as expenditure. While such instruments are not universally applicable, they can play a catalytic role where enabling conditions exist.
Conclusion: Repositioning Health at the Core of Africa’s Transformation Agenda
Africa stands at a critical juncture. The continent has a unique opportunity to leverage frontier technologies to accelerate productivity growth and structural transformation. However, this opportunity will remain constrained unless foundational investments in human capital—particularly health—are addressed.
Current health financing systems are insufficient, unequal, and unsustainable. Without decisive action to expand fiscal space, improve spending efficiency, and deploy appropriate financing instruments, the productivity gains required for transformation will remain out of reach.
Repositioning health within macroeconomic policy frameworks is therefore essential. This requires moving beyond a narrow sectoral perspective and recognizing health as a core driver of productivity, resilience, and long-term growth.
Only through such a shift can Africa close the loop—from growth without productivity to productivity-led structural transformation.